This
blogpost about ethics in international development is about a randomised control trial (RCT) in Kenya. In the experiment, some households in Kenya were given unconditional cash transfers of either USD 404 or USD 1525. The researchers found, unsurprisingly, that the lucky ones were happier and that their unlucky neighbours were unhappy. The paper is aptly titled
“Your Gain is my Pain”.
Most importantly, however, the blogger reflects on why this type of research is done at all:
"Am I the only one to think that is not ethical dishing out large sums of money in small communities and observing how jealous and unhappy this makes the unlucky members of these tight knit communities?"
For myself, as a development practitioner with a systems thinking perspective, RCTs can come across as having very limited usefulness and application. They can also be quite machine-based: they either choose to wilfully ignore human behaviour or they simply limit their interactions with other disciplines (psychology, sociology, anthropology) so that they can create more simple hypotheses. Thus, it is felt that the applicability of an RCT for complex problems (such as systemic poverty) is limited.
The RCT we have seen from Kenya seems to fall into that trap too. This RCT seems to need to test the notion that poor people in Kenya might not exhibit the same reactions and behaviours as other people. As if the nature of the human condition (in Africa) is under exploration. To me, this is strange and feels like the original hypotheses might have been drastically distilled and reduced down to overly simplified thoughts.
I wonder how the findings would actually be useful to policy and projects. Who might need proofs from an RCT that Kenyans are like any other human being? How could such research be useful for development planning at an economic or social level? Why is the notion that proving that desperation, jealously and unhappiness occurs among very poor people is valuable? I would also wonder what long-lasting impact this type of research would have on social relationships in the communities in the future.
Globally, there is a large community of development practitioner who feel that RCTs in poverty interventions are not ethical and not useful. From my conversations with them, they make the following points:
- In many RCTs, an assumption is made that the the groups will not be communicating with each other. However, it is actually very difficult to have demarcated and clear boundaries for the treatment groups to be adequately isolated. People talk. Information can flow through multiple channels and through multiple mechanisms (face-to-face, mobile phone, internet, etc) across groups, geographies, social hierarchies, institutions, etc.
- In RCTs, people might be very desperate because of the psychological and social impact of poverty and crisis. In this case all the RCT does is exacerbate that desperation and exacerbate those behaviours that present themselves when people are in desperate situations. The results are therefore naturally biased and skewed and outlying when compared to any group at any point in time. This is not adequately recognised in RCTs and thus not at all reflected when RCTs attempt to influence policy and project applications.
- Over time, the RCT can have a lasting negative impact. Those RCTs which test the type of reactions as the one featured here in Kenya - jealousy and unhappiness - can damage social relationships between individuals and groups even after the trial has ended. Real people are not as adept to switching off their pain and trauma (and any additional feelings of betrayal, anger, envy, frustration, etc.) as machines might be able to!

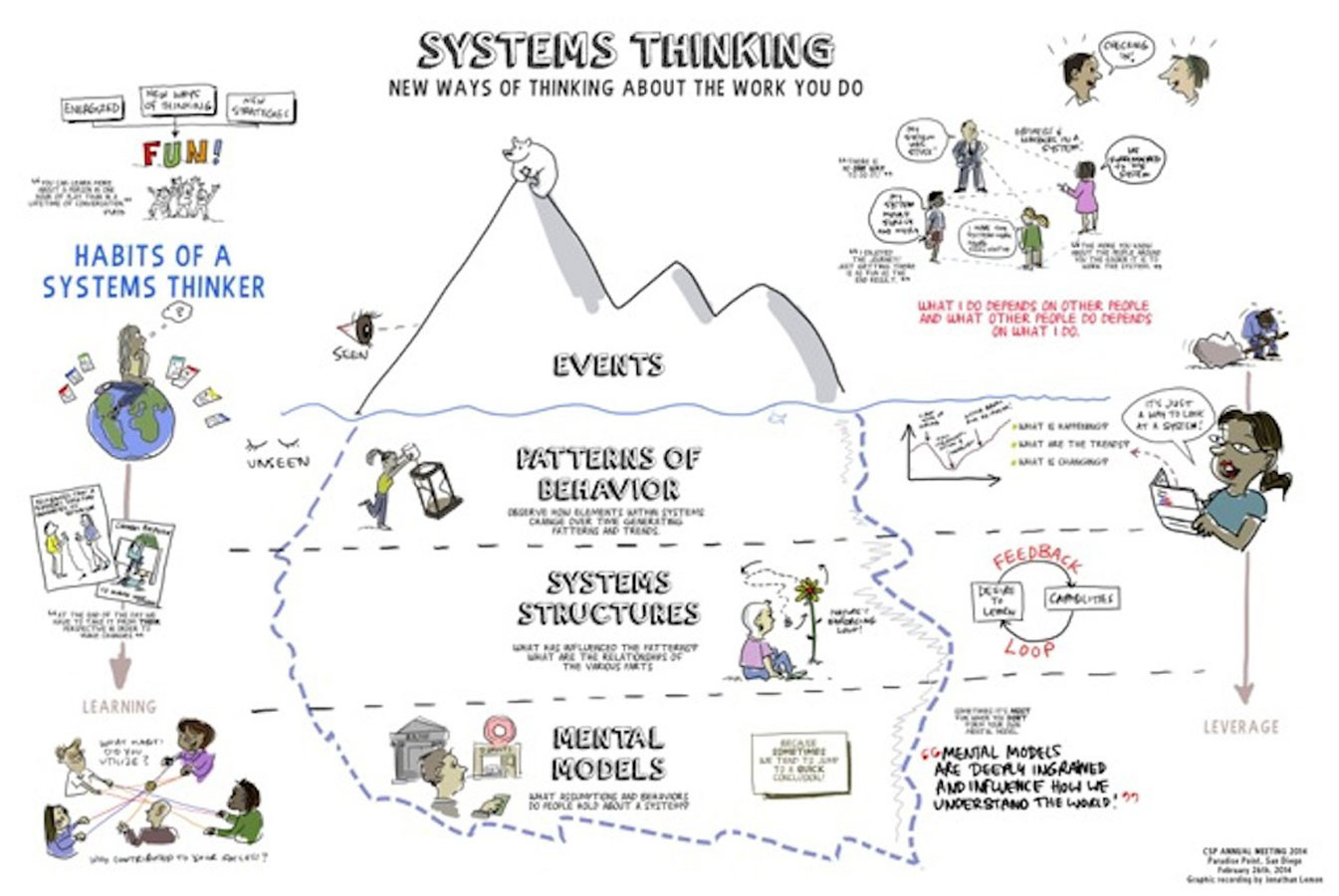
 , which shows some common skills associated with systems thinking.
, which shows some common skills associated with systems thinking.